



What were you doing in 1999?
In 1999, MSF launched the Access Campaign out of medical necessity and frustration. MSF staff in the field were facing multiple challenges – unable to provide adequate treatment to people dying from HIV/AIDS, tuberculosis, malaria, and neglected tropical diseases because new or existing drugs were priced out of reach; were ineffective, toxic, or ill-adapted for use in the places we work; or simply did not exist at all.
Els Torreele, Executive Director, MSF Access Campaign
“The multinational pharmaceutical industry has wielded unchecked pricing power… that prioritises profits over people’s health.”

These deficiencies were not due to scientific or technical limitations. They were the result of conscious political choices about how medical innovation and access to health tools are organised and financed globally.
Rooted in an economic and political system put forth by wealthy governments, the multinational pharmaceutical industry has wielded unchecked pricing power through patents and other monopolies, imposed globally through trade laws that prioritise profits over people’s health. “Medicines shouldn’t be a luxury” has been, and remains, the Campaign’s most poignant rallying cry.

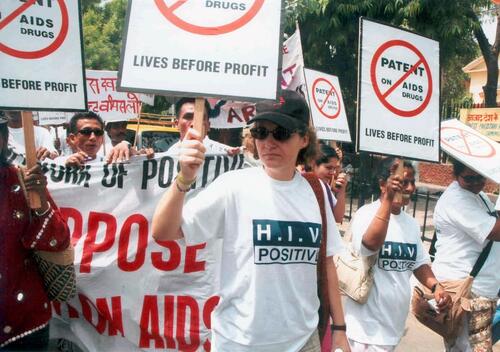
The Campaign’s initial priority was on overcoming barriers to accessing lifesaving HIV antiretroviral drugs, then sold at more than US$10,000 per person per year. Together with patient activists, MSF spoke out about the fundamental injustice of letting people with HIV/AIDS die because they cannot afford the deliberately high prices companies charged for medicines.
An emerging access-to-medicines movement put pressure on pharmaceutical corporations, governments and other ‘powers that be’ to crack this deadly gridlock and obtain lower drug prices to increase access to HIV treatment.
It worked. By overcoming the companies’ monopolies and fostering generic production and competition, the price of antiretroviral drugs dropped 99% over the next decade, paving the way towards scaling up treatment for people living with HIV/AIDS to over 22 million at the end of 2018.

1998
Frustration catalyses into action
In the late 1990s, frustration mounts over people dying from treatable diseases. MSF begins to document the problem, joining with patient groups to speak out forcefully and demand action. To overcome Pfizer's price gouging, we campaign for Thai drug companies to be able to produce affordable versions of fluconazole, used to treat dangerous infections in people with HIV/AIDS. And we publicly denounce pharmaceutical company Roussel for abandoning production of a key treatment for meningitis.
1999
Access Campaign launched
MSF’s Campaign for Access to Essential Medicines, now the Access Campaign, is publicly launched. A small team works to analyse and overcome the underlying barriers that prevent people from accessing treatment, including patent, intellectual property and trade rules, and research and development (R&D) policies. When MSF is awarded the Nobel Peace Prize in October, the funds go towards efforts to improve treatments and boost research for neglected diseases.

2000
Breaking rules to save lives
Frustrated MSF teams in Thailand decide to break rules against importing HIV medicines so they can treat people dying of AIDS. MSF works with patient groups to set up a ‘buyers club’, shipping medicines via Myanmar to avoid detection. We also support civil disobedience, led by the Treatment Action Campaign, to defy patent laws to import affordable generic medicines into South Africa, an epicentre of the AIDS epidemic, leading to price concessions from Pfizer.

2000
Price reductions for TB drugs
MSF works with World Health Organization (WHO) and other partners to reduce the exorbitant price of drug-resistant TB (DR-TB) medicines – up to US$14,000 per treatment course – by negotiating discounts for five key medicines. But DR-TB remains exceedingly difficult and expensive to treat, with severe side effects and dismal cure rates. We are still campaigning for more effective, affordable TB treatments.

2001
Big Pharma vs Nelson Mandela
A 1997 lawsuit by 39 drug companies against the South African government threatens to block imports of low-cost, generic treatments for HIV/AIDS and other diseases. Over several years, South African activists mount protests, defiance campaigns and legal actions to oppose the lawsuit, and 300,000 people from 130 countries sign MSF’s international “Drop the Case” petition. In April, facing a public relations disaster of global proportions, Big Pharma announces they will unconditionally drop their legal case.

2001
Landmark price for HIV treatment
2001 marks a radical shift in the political feasibility of treating HIV/AIDS in developing countries. One year prior, MSF’s claim that 3-in-1 combination antiretroviral therapy could be as low as US$200 per person per year was met with widespread disbelief. But in February, Indian generic manufacturer Cipla publicly offers MSF a price of $350 per year, a huge drop from Big Pharma’s $10,000 price tag. Competition sparks further price reductions in the years that follow.

2001
Political shift for HIV/AIDS response
Several other events in 2001 lead to a political shift that catalyses the global response to HIV/AIDS. UN Secretary-General Kofi Annan calls for a “war chest” of $7-10 billion to fight infectious diseases; this later becomes The Global Fund to Fight AIDS, Tuberculosis and Malaria. The UN convenes an historic Special Session on HIV/AIDS, the first such meeting devoted to a health issue.

2001
Doha Declaration reaffirms health over commerce
Having identified patent monopolies as a major barrier that prevents access to affordable medicines, MSF and others campaign for the World Trade Organization (WTO) to explicitly confirm governments’ legal rights to implement patent and trade laws in a way that protects public health and promotes access to medicines. In November, the WTO adopts the Doha Declaration, reaffirming the existence of public health safeguards in international trade rules.

2001
Reviving treatments for Sleeping sickness
In the late 1990s, the few drugs that could be used to treat sleeping sickness, which is fatal without treatment, were at risk of going out of – or had already gone out of – production, with companies saying they weren’t profitable. After lengthy negotiations with MSF and WHO, Aventis agrees to resume production of eflornithine. MSF also helped get Bayer to restart production of two other drugs used to treat the disease.

2001
Chronic crisis in R&D for neglected diseases
An independent group of experts convened by MSF, the Drugs for Neglected Diseases working group, publishes seminal research showing only 1% of drugs new drugs approved from 1975-1999 were for neglected tropical diseases, which represented 12% of the global disease burden. Defining the crisis as a result of both market and public policy failures, the report makes several recommendations, including exploring a new initiative for collaborative, not-for-profit drug development focused on neglected diseases.

2003
'ACT Now' campaign for malaria
MSF’s ‘ACT Now’ campaign urges countries to switch to more effective malaria treatment: artemisinin-based combination therapy (ACT). This followed new recommendations from WHO, which came after MSF studies in sub-Saharan Africa helped confirm the extent of resistance to older malaria treatments. The campaign calls on international donors to fund ACT and appeals to African governments to roll out ACT as quickly as possible.

2003
Drugs for Neglected Diseases initiative
MSF and partners launch the Drugs for Neglected Diseases initiative (DNDi), an independent, non-profit drug development organisation focused on developing new treatments for some of the world’s most neglected diseases. Over the next 15 years, DNDi goes on to deliver eight new treatments for five deadly diseases - malaria, sleeping sickness, Chagas disease, leishmaniasis, and paediatric HIV.
2005
India moves to protect affordable medicines
Obliged by the World Trade Organization to start patenting drugs in 2005, India decides to put protections in place to protect public health and prevent patent abuse. Ever since, pharmaceutical corporations and some governments have sought to undermine India’s ‘section 3(d)’ law. MSF continues to work alongside civil society to fend off attacks and protect India’s role as the ‘pharmacy of the developing world’ that MSF and millions of people beyond our programmes rely on.

2006
Challenging patents to lower prices
To overcome exorbitant prices for critically important HIV medicines, the Thai government authorises local production of affordable versions of efavirenz and lopinavir/ritonavir by overriding blocking patents, and Brazil follows suit for efavirenz. For the first time, MSF supports a legal challenge to a patent, for HIV drug tenofovir, to increase access to lower-priced generics.

2006
Novartis targets 'pharmacy of the developing world'
Swiss drug company Novartis takes legal action in India to gut the country’s section 3(d) patent law. A Novartis victory would effectively cut the lifeline of affordable newer medicines from India upon which millions of people rely. MSF’s campaign, “Novartis, Drop the Case!”, collects nearly half a million signatures, including from Archbishop Desmond Tutu. Novartis loses the case and appeals the decision all the way to the Supreme Court, but the decision against the corporation is finally upheld in 2013.

2007
Better nutrition for children in crisis
In the early 2000s, use of therapeutic ready-to-use foods revolutionised treatment of severely malnourished children. By 2007, MSF is using nutritionally-enhanced supplements on a large scale to prevent malnutrition in at-risk populations. MSF campaigns for a global scale-up of nutrient-rich foods to prevent and treat childhood malnutrition; by 2010, their use is a cornerstone of humanitarian response. MSF’s next campaign, “Starved for Attention,” pushed the US government to improve the nutritional quality of conventional food aid.

2009
A new route to affordable HIV medicines
To accelerate access to more affordable HIV/AIDS medicines, MSF proposes and then campaigns for the creation of a new initiative to encourage and facilitate drug companies to license production to generics manufacturers. The Medicines Patent Pool is established in 2010 and its first license is signed the same year. The Pool subsequently opens for licensing of TB and hepatitis C medicines.

2010
Hands Off our Medicines!
MSF’s “Europe! Hands Off Our Medicine” campaign demands removal of harmful provisions from the EU-India trade agreement, which threatens the supply of affordable medicines made in India. For years, MSF has advocated to remove harmful intellectual property and patent rules that restrict access to medicines from international trade agreements. MSF and civil society continue to mobilise under the ‘Hands Off Our Medicines’ campaign in support of developing countries’ legal rights to protect access to affordable medicines.

2012
Test Me, Treat Me: a DR-TB Manifesto
The “Test Me, Treat Me” DR-TB Manifesto gives voice to people affected by drug-resistant TB and demands political and financial support for better diagnosis and treatment. 55,000 people sign the Manifesto written by Phumeza Tisile, who was treated for XDR-TB in MSF’s clinic in Khayelitsha, South Africa, and her MSF doctor Jenny Hughes. In May 2014, Phumeza addresses the World Health Assembly as governments approve an ambitious 20-year global plan to curb the TB epidemic.

2014
Empty-handed for Ebola epidemic
When MSF responds to the West Africa Ebola outbreak that eventually kills 11,000 people, we have no vaccine, no treatment and no simple diagnostic test. MSF decries the lack of R&D investment and supports the creation of a new vaccine initiative, Coalition for Epidemic Preparedness Innovations (CEPI). MSF continues to push for all new tools to be affordable and adapted for use in endemic countries.

2015
A Fair Shot campaign for affordable vaccines
MSF's “A Fair Shot” campaign kicks off, calling on Pfizer and GSK to reduce the price of the pneumonia vaccine – the most expensive standard childhood vaccine – to $5 per child. In 2016, a price of $9 per child is offered to humanitarian organisations like MSF, for use in emergencies. But millions of children are unvaccinated in countries where the vaccine is still too expensive; we continue to demand an affordable price for all developing countries.

2017
Price drops for hepatitis C medicines
Today’s hepatitis C medicines are very effective, but high prices have prevented access, especially in middle-income countries. MSF and other civil society groups challenged patents and pressured pharmaceutical companies to reduce prices; in 2017, MSF obtains a price of $120 per 12-week treatment – less than a tenth of what we had been paying, and a fraction of the commercial launch price of $147,000. As MSF scales up hepatitis C treatment, we want all governments to access the same low price.

2018
Breakthrough for sleeping sickness
A result of 10 years research efforts from discovery to clinical development, DNDi launches a new oral drug for sleeping sickness, fexinidazole, fulfilling a longstanding medical need identified by MSF years ago. This breakthrough shows that a collaborative, not-for-profit and public-interest approach to medical R&D can deliver effective new treatments that put patient needs ahead of financial gains.
1998
1999
2000
2001
2003
2005
2006
2007
2009
2010
2012
2014
2015
2017
2018
Other successes followed, from increasing access to rapid diagnostic tests and artemisinin-based combination treatments for malaria, to decreasing the prices of the pneumococcal conjugate vaccine and hepatitis C drugs, and fostering research and development (R&D) for the most neglected diseases – including the creation of the Drugs for Neglected Diseases initiative (DNDi), who are now celebrating the launch of fexinidazole, a new all-oral cure for African sleeping sickness.
Each advancement reflects the unique multidisciplinary nature of the Campaign. Our staff combine technical and political analysis based on MSF medical data and operational experience together with strategic advocacy in partnership with allies worldwide – all to get adequate health tools to people who need them most, as well as catalyse broader systemic change so we do not need to keep fighting the same access battles over and over again.
The crisis of access to medicines and innovation is no longer one of only ‘poor people’ in developing countries, but a truly global one. Our slogan “Medicines Shouldn’t Be a Luxury” is valid for people all over the world.Els Torreele, Executive Director, Access Campaign
But where do we stand today, 20 years on?
Unfortunately, despite winning some battles, the access-to-medicines challenges are larger than ever, with many new drugs, diagnostics and vaccines marketed at increasingly high prices, monopolies more entrenched, and pharmaceutical corporate powers more globalised.
At the same time, we are missing the tools we need to control rising antimicrobial resistance and outbreaks of epidemic diseases such as Ebola.
But herein lies an opportunity. The crisis of access to medicines and innovation is no longer one of only ‘poor people’ in developing countries, but a truly global one. Our slogan “medicines shouldn’t be a luxury” is valid for people all over the world, and finding solutions is a topic of public and political debate in wealthy and developing countries alike.

Video
Access Campaign - Lives Over Profit
In this ever-changing world, we are advocating for needs-driven medical R&D and access as a collective responsibility, with the results of this concerted effort considered as a public health commons, with collective right of use.
Given that medical R&D is largely financed by public funds, it is unacceptable that unchecked monopolies are privatising and financializing this common scientific progress, while health systems collapse under the financial burden and people die for lack of medicines. Access to health, including medicines, is a matter of justice, not charity.
Marking the 20th anniversary of the Access Campaign provides an opportunity to look back on what we’ve learned, reflect on this new reality, and carve out new ways for MSF to engage in transforming the medical innovation and access ecosystem to better address the health needs of people in our care.
What will you be doing in 2019 and beyond to help us achieve this shared goal?
![Wishlist 2020 - FUTURE [Twitter version]](https://img.msf.org/Docs/MSF/Media/CMS3/0/9/8/6/MSF298431.jpg "Wishlist 2020 - FUTURE [Twitter version]")
Access to medicines
Our 2020 wishlist - five New Year's resolutions for medical care
Campaign
22 Jan 2020

Access to medicines
Gavi must ensure more children get new, more affordable pneumonia vaccine
Press Release
21 Jan 2020

Nigeria
Medical assistance urgently needed outside northeast ‘garrison’ towns
Interview
19 Dec 2019